Have you ever experienced food getting stuck in your throat when you swallow? Most of us quickly get over any such scary moment as coordinated muscle contractions (peristalsis) propel the food down into the stomach. However, for those with a rare condition called achalasia, swallowing difficulties are a chronic problem.
Achalasia affects an otherwise smooth and natural operation of the oesophagus, the tube connecting the mouth and the stomach. Globally the condition affects about 10-20 people out of 100,000 people.
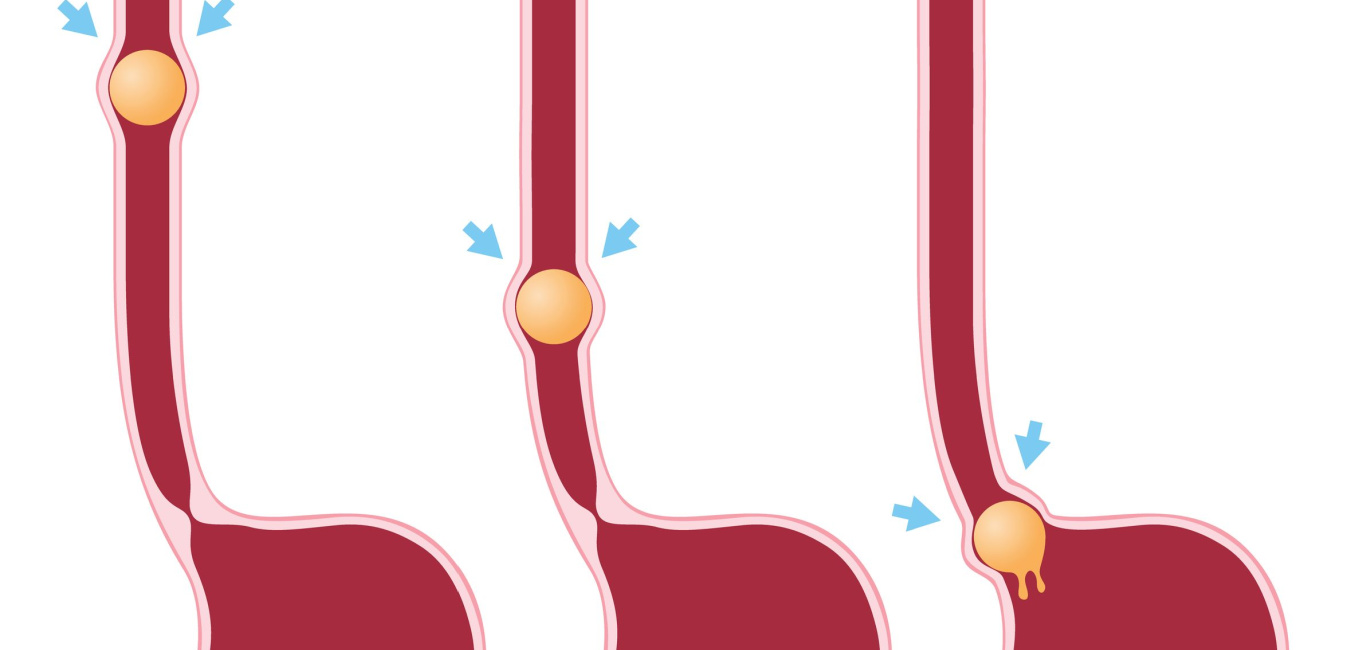
According to Dr Piyush Ranjan, senior consultant at New Delhi’s Gangaram Hospital, achalasia occurs when the oesophageal muscles do not squeeze food down; the muscle valve called the lower oesophageal sphincter (LES) fails to relax. As a result, food gets trapped in the oesophagus instead of entering the stomach.
While the exact cause remains unknown, achalasia stems from the destruction of certain inhibitory neurons that produce nitric oxide, a molecule that relaxes oesophageal muscles. When the LES does not relax as a result, food cannot enter the stomach and will get stuck in the oesophagus, explains Dr Ranjan.
Symptoms of achalasia
The condition manifests as a range of symptoms primarily attributed to compromised peristalsis and sphincter closure:
- Dysphagia: Difficulty in swallowing solids and liquids persisting over a long period
- Regurgitation: Food going up from the oesophagus and re-entering the mouth
- Chest pain
- Heartburn
- Fatigue
- Malnutrition
- Weight loss
- Liquids entering the airways
- Nocturnal cough
“People often mistake these symptoms for acid reflux or gastroesophageal reflux disease (GERD), delaying the diagnosis of achalasia,” Dr Ranjan observes.
In rare cases, a long-standing achalasia can potentially lead to oesophageal cancer. It may also result in diverticulum or out-pouching of the oesophageal wall in the long term, he adds.
Diagnosing the problem
Achalasia is diagnosed after thorough clinical examination followed by specific tests, as Dr Ranjan outlines here:
- An endoscopy rules out other causes of swallowing difficulty, such as cancer at the lower end of the oesophagus. Persons with achalasia will have a dilated oesophagus, along with a puckered sphincter, the obstructed food and saliva.
- Oesophageal manometry is the gold standard to diagnose achalasia. It measures the pressure in the lower end of oesophagus and LES. An increase in pressure above the normal confirms achalasia.
- Barium swallow test is an alternative test when manometry facilities are lacking. The person swallows a solution having barium, followed by an X-ray. It shows a bird’s beak-like appearance due to the narrowing of the oesophagus.
Dr Ranjan notes that comprehensive diagnosis involves an endoscopy followed by an oesophageal manometry.
Coping with achalasia
“At present, there’s no cure for achalasia,” he says. “Current treatments focus on alleviating symptoms by reducing LES pressure, clearing obstructions and aiding oesophageal emptying into the stomach.”
Treatment includes the following options:
- Endoscopic /pneumatic dilatation: A 15-minute procedure uses a balloon to dilate the LES and provides temporary relief, but recurrence is common.
- POEM or per oral endoscopic myotomy: The oesophageal muscle is cut internally. The procedure is considered the most effective endoscopic treatment with long-lasting results.
- Heller’s myotomy: Surgical removal of the oesophageal muscle, performed with an abdominal incision.
- Botox or botulinum toxin: commonly used in certain cosmetic treatments – is given in the LES for temporary relaxation. It is given usually to immobile and moribund individuals. The effect of a Botox injection, however, is short-lived.
- Medication: Certain medications are also used to relax the LES, although with limited efficacy.
In an estimated 10 to 15 per cent of cases, acid reflux may occur after surgery. However, Dr Ranjan says it can be managed with medications or additional procedures.